Landscape of Opportunity

Introduction
California’s communities of color have long faced persistent health disparities arising from structural and racist inequities that block access to the resources and opportunities needed to maintain good health. Key among these inequities include a safety net that still fails to provide every person with their basic needs for health care, nutrition, and housing.
Although federal and state legislation including the Affordable Care Act (ACA) and Medi-Cal expansions for undocumented youth have greatly improved the safety net’s reach, these solutions are not enough to close these disparities. Care access remains poor, especially for immigrant and limited English proficiency populations, and communities of color also continue to experience disparities in their health outcomes.
These disparities take place in the context of a changing California. Already, over half of all Californians identify as non-white, highlighting the importance of closing these long-standing inequities. And the COVID-19 pandemic has increased the urgency of this task, exacerbating long-standing disparities, leading to disproportionate harm among communities of color.
The Landscape of Opportunity provides an overview of the current state of health disparities and challenges facing California’s communities of color. It serves as a resource for advocates and policymakers alike, highlighting the key areas where disparities persist that are ripe for future action to advance health equity.
Section One: California’s Diverse Communities
California’s diversity contextualizes the urgent needs and opportunities to advance health equity. As the nation’s most diverse state, California represents a wide array of communities made up of diverse races and ethnicities who speak many different languages. As the State moves to address long-standing health disparities and challenges, it must account for the varied and specific needs of these communities, ensuring that no one is left behind.
Communities of Color Make Up Over Half of California’s Population
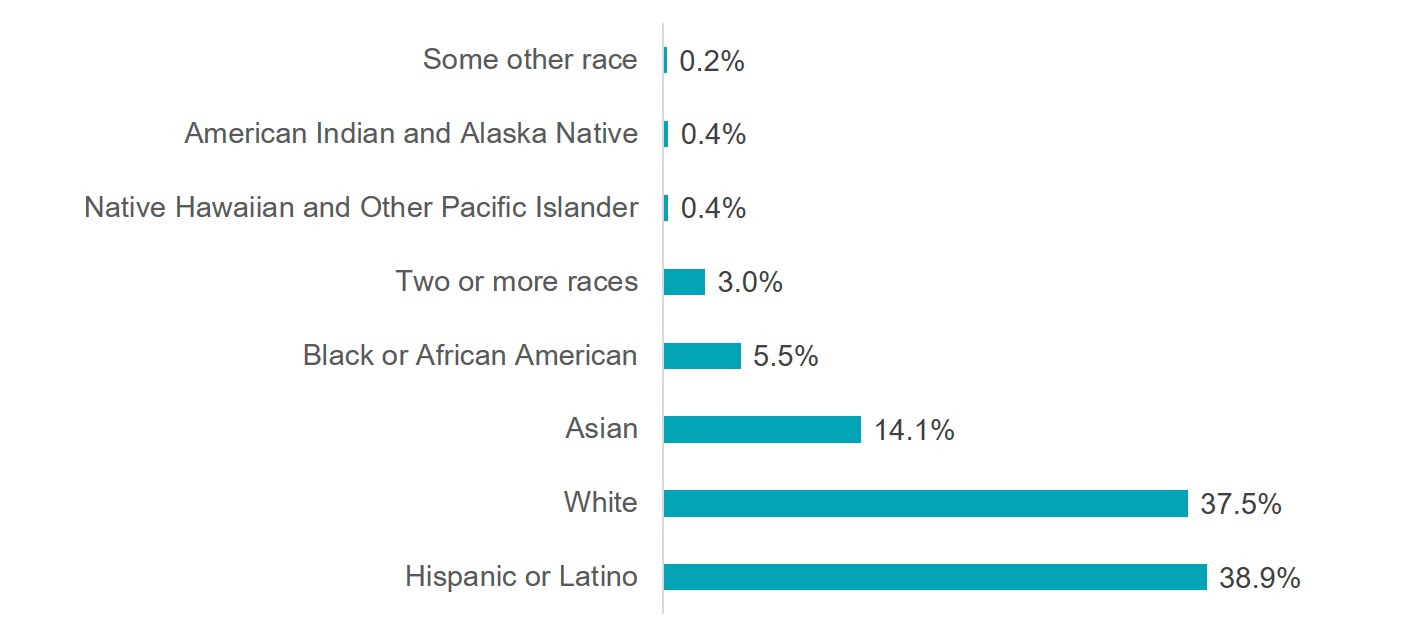
Communities of color compose 63% of the population in the state. The counties with the highest percentage of communities of color are Imperial (89%), Los Angeles (74%), and Merced (72%).
Californians Speak Many Languages

46% of Californians speak a language other than English at home. In addition, 18.1% of Californians over age 5 have limited English proficiency. The counties with the highest percentage of individuals with limited English proficiency are Imperial (33%), Monterey (28%), and Tulare (27%).
California is Home to Many First-Generation Immigrant Families
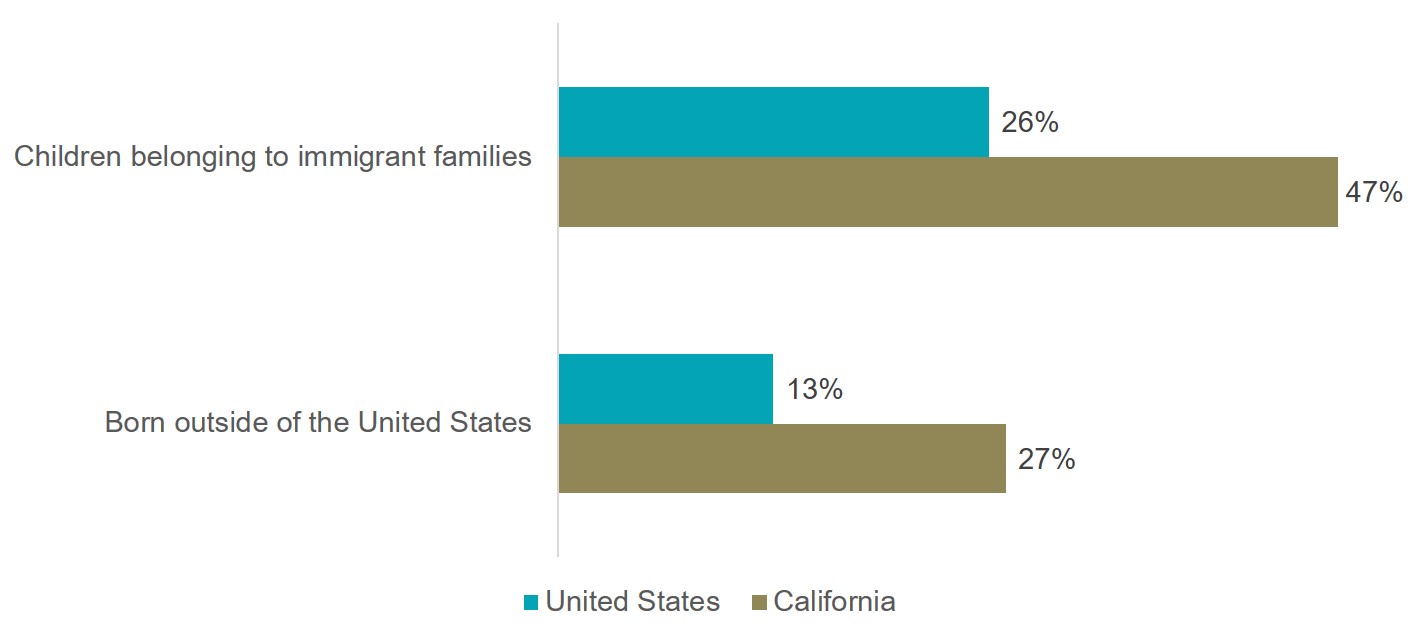
California has a robust immigrant community that spans for generations. 26.9% of the state’s population are first-generation immigrants (born in another country and migrated to CA), and 47% of all children belong to an immigrant family (at least one parent born outside of the country).
In comparison, 13% of residents nationwide are first-generation immigrants, and only 26% of children belong to an immigrant family.
Source: Migration Policy Institute Data Hub; U.S. Census Bureau American Community Survey
Section Two: Systemic Racism in Health Outcomes
Communities of color face persistent health disparities including higher rates of asthma, diabetes, and obesity, resulting in a shorter life span, less wealth, and less opportunity. These disparities cannot be attributed to any inherent characteristics of these communities – they are the product of structural and racist inequities that block access to resources and opportunities.
Communities of Color Experience Worse Health Outcomes
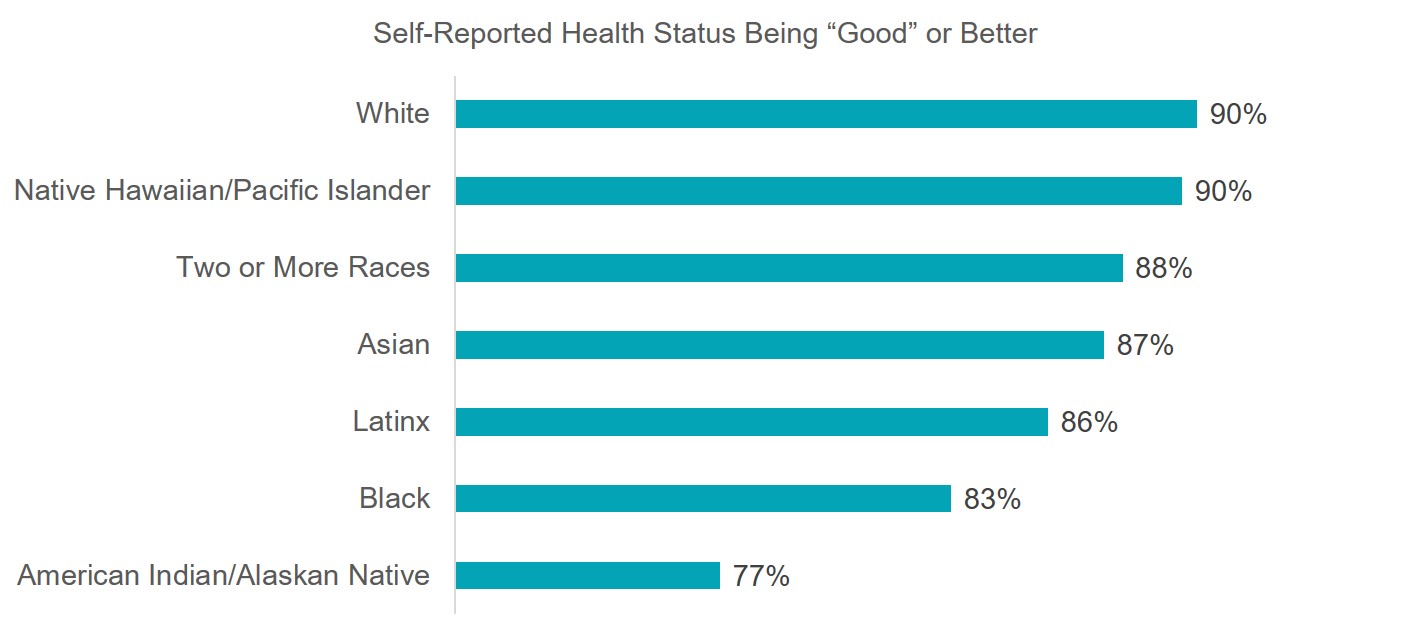
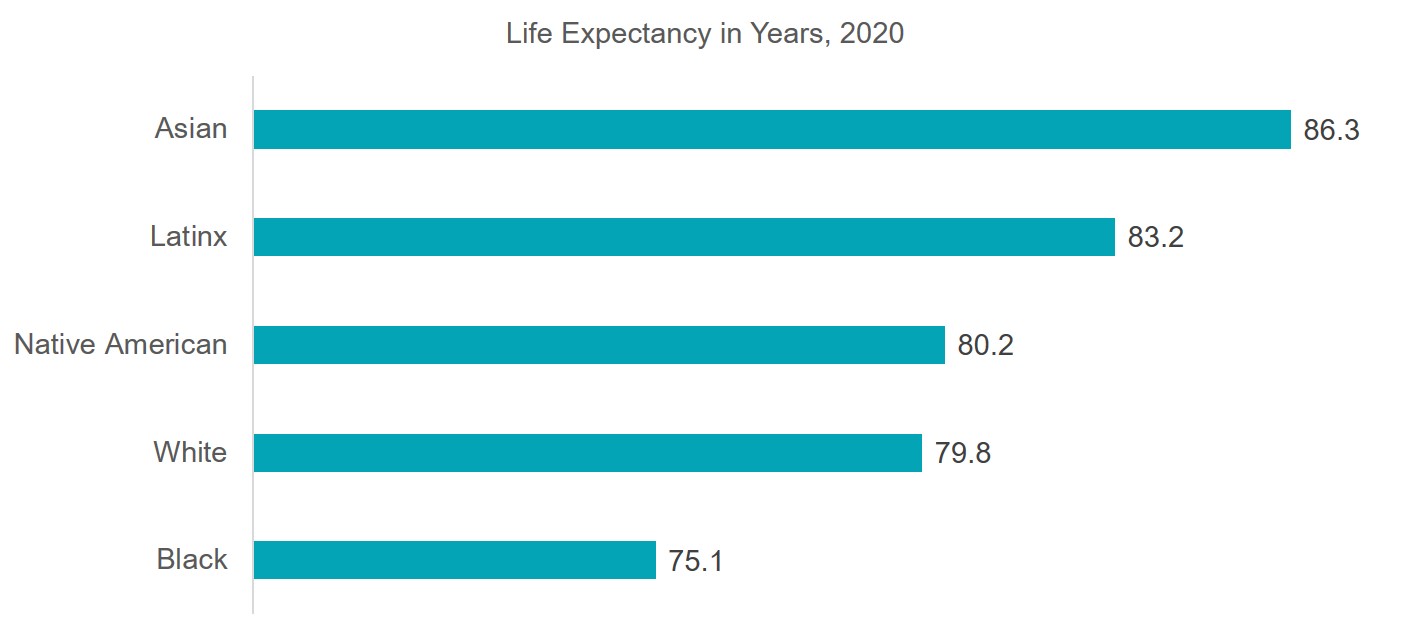
Communities of color self-report worse health outcomes than white people. Though life expectancy shows many communities of color having higher life expectancies than white people, the discrepancy between health status and life expectancy can show communities of color living longer with worse health conditions/outcomes.
The Black community reports one of the lowest health outcomes while having the lowest life expectancy at 75.1 years of age.
Source: California Health Interview Survey; World Population Review
Communities of Color Experience Higher Rates of Chronic Health Conditions: Diabetes
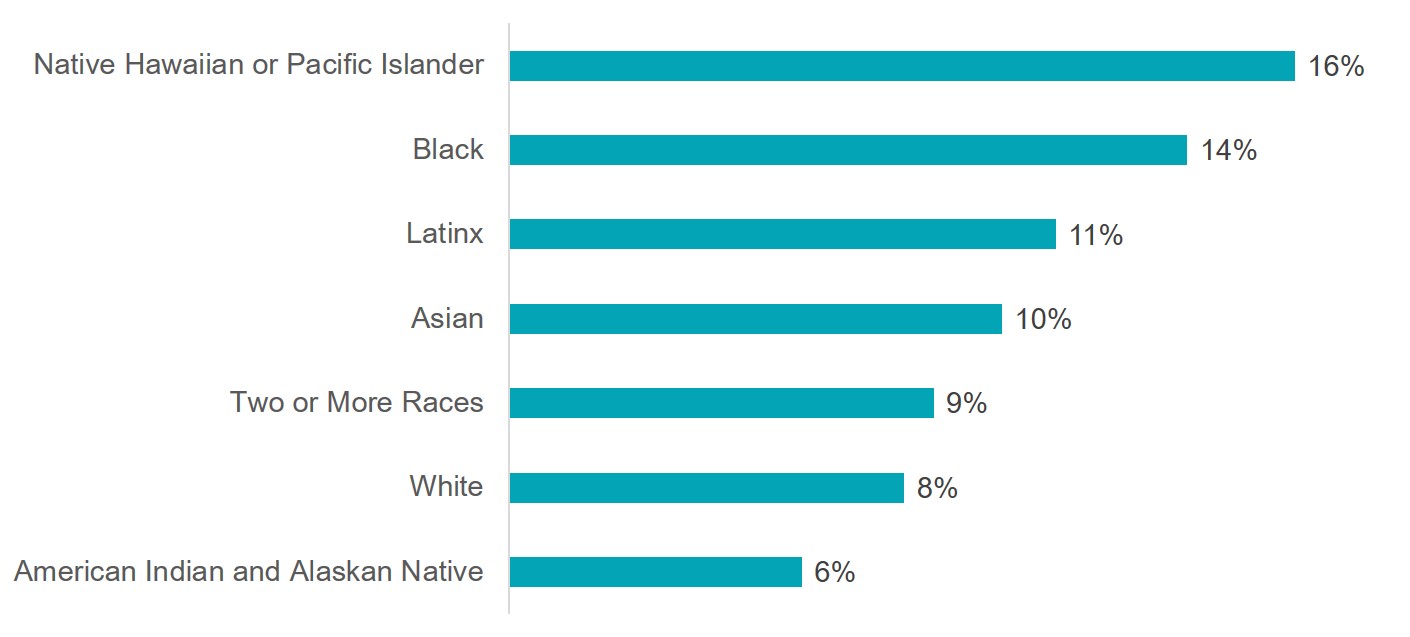
Native Hawaiian and Pacific Islander communities experience double the rates of diabetes than white people. Black, Latinx, Asian, and multiracial communities all report higher incidences of diabetes than white people. Prevalence of chronic health conditions like diabetes can be further exacerbated by limited and costly options to healthier food options and limited space and opportunity for physical activity.
Communities of Color Experience Higher Rates of Chronic Health Conditions: Asthma

There are three communities of color that report higher rates of asthma: American Indian or Alaska Native, multiracial communities, and Black communities. American Indian or Alaska Natives have nearly double the asthma rates of white people. Incidences of asthma can signal socioeconomic or environmental conditions that could lead to increased cases.
Section Three: Systemic Racism in Health Care Delivery
A health care delivery system that is not grounded in racial equity will result in racial disparities. Presently, communities of color represent a majority of Medi-Cal enrollee. However, communities of color are but are still more likely to be uninsured or underinsured. Moreover, crucial needs like mental health care and dental care continue to be unmet, even when health care delivery systems like Medi-Cal count these two benefits as part of their comprehensive coverage for adults.
Communities of Color Are the Majority of Medi-Cal Enrollees

At 80.7%, communities of color compose the majority of Medi-Cal enrollees. The largest enrollee group are Latinx members, who make up 57.7% of enrollees. The second largest group comprises white members who make up 19.3%, and the third are Asian members who make up 11.7% of enrollees.
Despite Experiencing Significant Gains Under The Affordable Care Act, Communities Of Color Still Lack Equitable Coverage Access
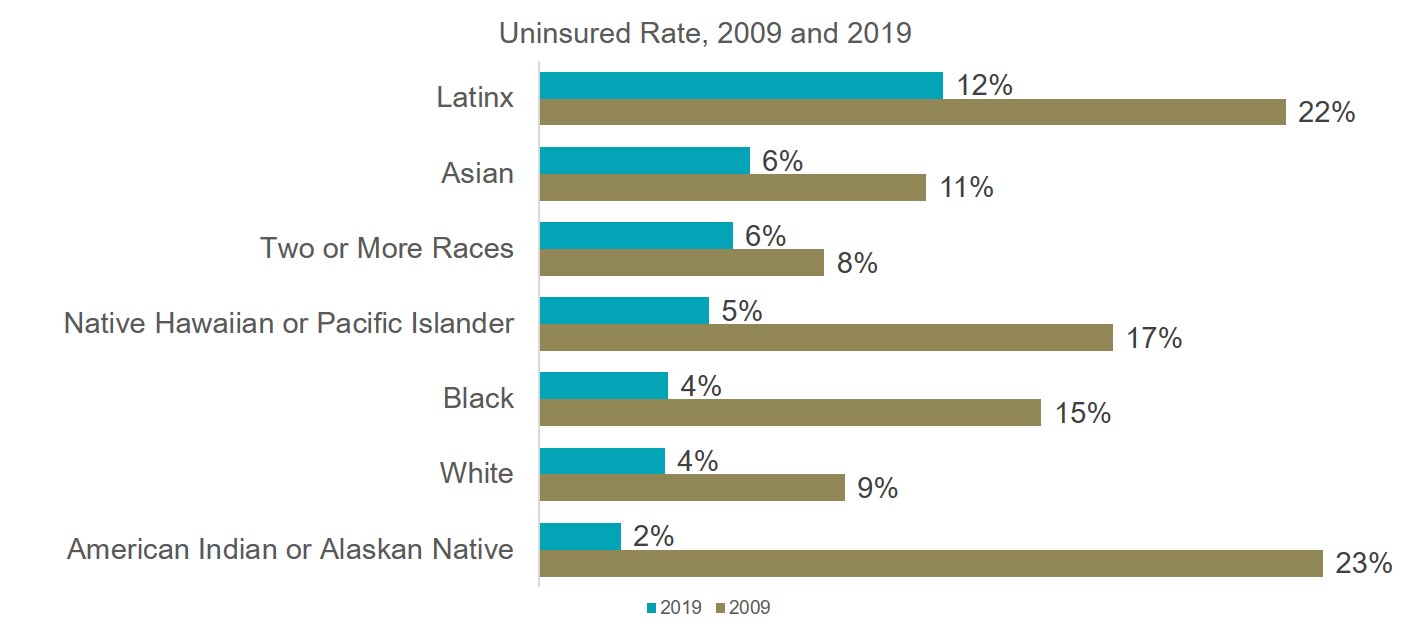
Due to the Affordable Care Act, there have been significant gains in healthcare coverage among communities of color. In 2009, a year before the passage of the Affordable Care Act, all communities of color reported higher uninsured rates than white people. Nearly all racial groups had well over a 10% uninsured rate, with Latinx and American Indians or Alaska Natives exceeding a 20% uninsured rate.
By 2019, the disparity diminished significantly across all races, but was not completely eliminated. American Indians and Alaska Natives saw the largest decrease in their uninsured rate, well under 5% uninsured. However, Latinx people remain the only group to exceed an uninsured rate of 10%, and most communities still experience uninsured rates greater than that of Whites.
Learn More: About the Affordable Care Act
Community Mental Health Needs are Significant; Yet Many Go Without Care
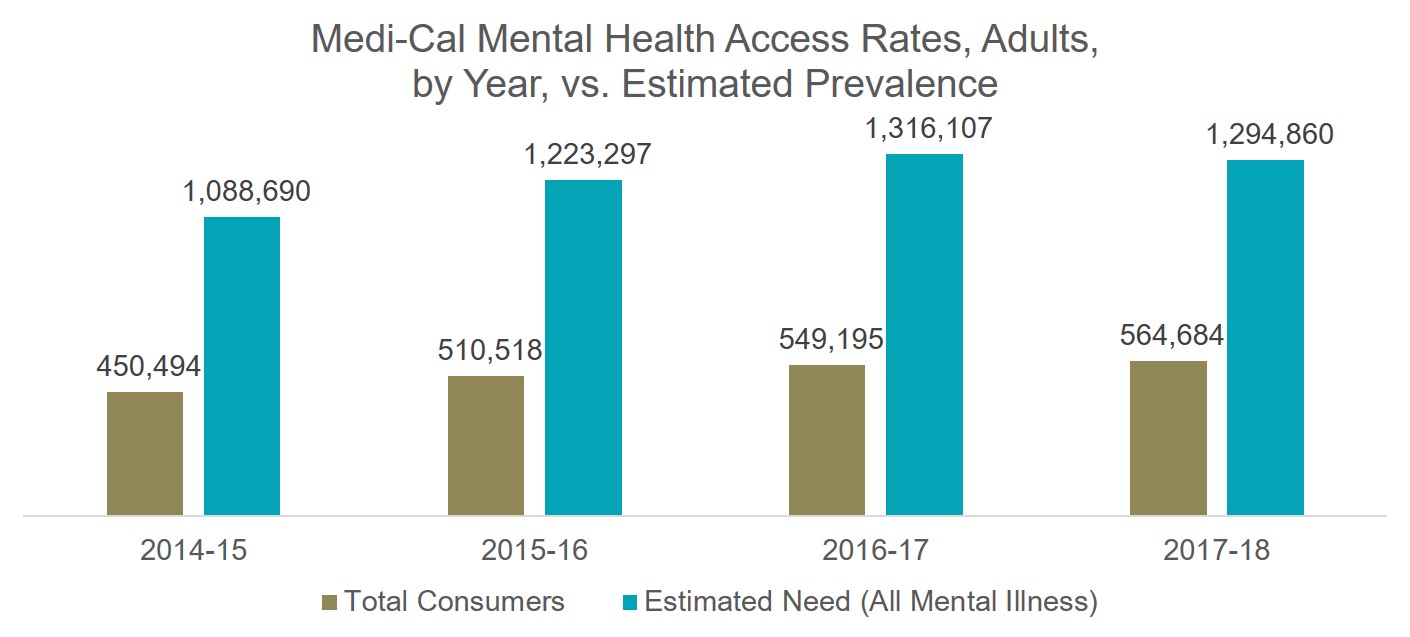
The need for mental health services by Medi-Cal beneficiaries continues to be unmet. The estimated number of enrollees with any mental illness has been more than double the amount of enrollees receiving mental health services from 2014-2018. Medi-Cal beneficiaries are entitled to comprehensive mental health benefits that include access to qualified mental health providers and psychiatric medication.
Source: Mental Health Disparities by Race and Ethnicity for Adults in Medi-Cal
Mental Health Access Rates Vary by Race/Ethnicity

And even though utilization of Medi-Cal mental health benefits is low across all demographics, racial disparities exist within the program. Nearly all racial groups utilize mental health services under their managed care plans at a lower rate than white beneficiaries. The lowest rate of usage within the managed care system is by Asian and Pacific Islander beneficiaries at 1.5%. Generally, managed care mental health services within the Medi-Cal program are for beneficiaries with mild to moderate levels of mental illness.
In comparison, there were only two racial groups that exceeded White access rates for County mental health services, Black and Alaskan Native or American Indian people. County mental health services are generally meant for more severe cases of mental illness.
It is important to note that Black people have one of the lowest access rates for mild to moderate, managed care use while they have the highest County Mental Health access rates.
Source: Mental Health Disparities by Race and Ethnicity for Adults in Medi-Cal
Dental Care Also Remains Out Of Reach For Many

In 2018, Senate Bill 97 restored adult dental benefits in the Medi-Cal program. The restored benefits included laboratory-processed crowns, posterior root canal therapy, periodontal services, and partial dentures, including denture adjustments, repairs, and relines. Although benefits have been restored for several years, racial disparities in access persist, and access rates remain low overall.
Geographic disparities also persist. For the 2018 calendar year, most of the state’s counties with eligible beneficiaries had a utilization rate above six percent. However, three counties had significantly low utilization rates. Out of Inyo county’s 3,542 adult beneficiaries, only 12 beneficiaries accessed dental care (0.34% of beneficiaries). In San Luis Obispo, 874 out of 38,034 adult beneficiaries accessed dental care (2.3% of beneficiaries). Also, Alpine had the lowest utilization out of all California counties, with zero adult beneficiaries out of 165 accessing dental care. Of California’s top three largest counties (Los Angeles, San Diego, and Orange), only San Diego exceeded 10% dental benefit utilization with 57,462 out of 539,026 adult beneficiaries accessing dental care in 2018. Out of Orange county’s 536,647 adult beneficiaries, 50,292 accessed dental care (9.37%), and in Los Angeles, 198,730 out of 2,391,307 (8.31%), adult beneficiaries accessed dental care.
Learn more: Hanging by a Thread
Source: Dental Utilization Measures and Sealant Data by County, Ethnicity, & Age Calendar Year 2013 to 2018
Section Four: COVID-19 Poses Urgent Challenges for Communities of Color
Though health disparities among communities of color existed before the Coronavirus pandemic, the public health crisis further exacerbated these disparities. Beyond the pandemic, anti-racist protests in the summer of 2020 delved the nation into discussions around historical racial discrimination, harm, and violence in many social sectors, including healthcare. Combined, we see the damage historical and persistent racism has on the health and security of communities of color.
COVID-19 Has Exacerbated Health Disparities
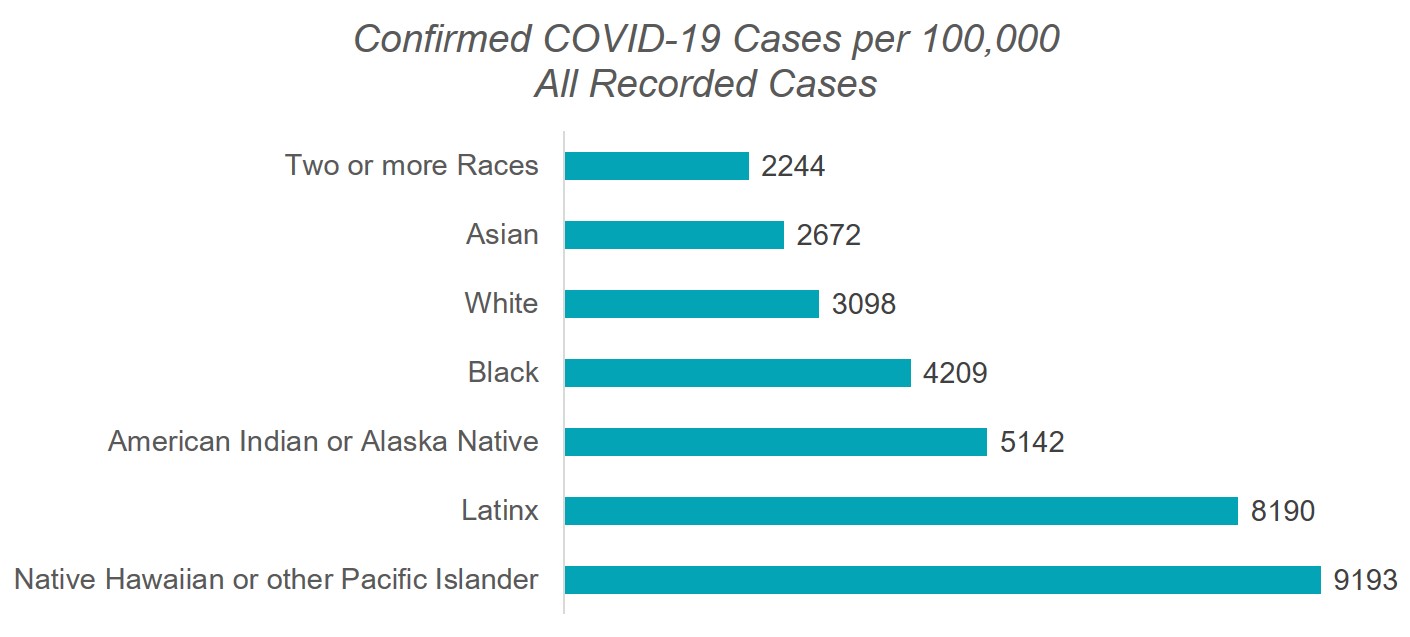

Latinx and Native Hawaiians or other Pacific Islanders have over three times as many cases of COVID-19 versus their white counterparts. Black people and American Indians or Alaska Natives have nearly double the cases over white people.
Although data for Asians suggests a lower case rate, disaggregated data that breaks apart the diverse ethnic groups classified as Asian is not available. Evidence suggests that the burden of COVID-19 is not borne evenly across Asian communities. For example, the Los Angeles Times reported that Filipino Americans were dying at a disproportionately high rate compared to other Asians. The Bulosan Center for Filipinx Studies also reported on the disproportionate impact of COVID-19 on undocumented and migrant Filipinos.
Source: U.S. Census Bureau American Community Survey; California Department of Public Health COVID-19 Race and Ethnicity Data; California’s commitment to health equity
Communities of Color Are Also Disproportionately Likely to Die From COVID-19
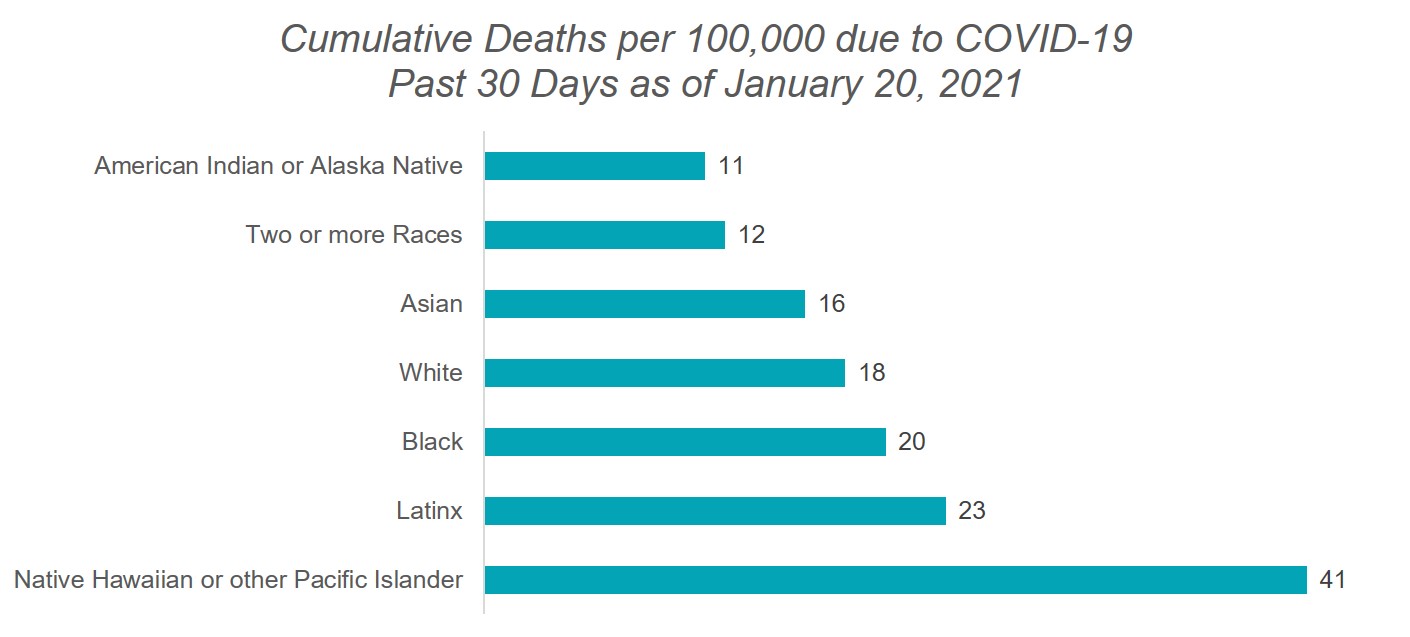
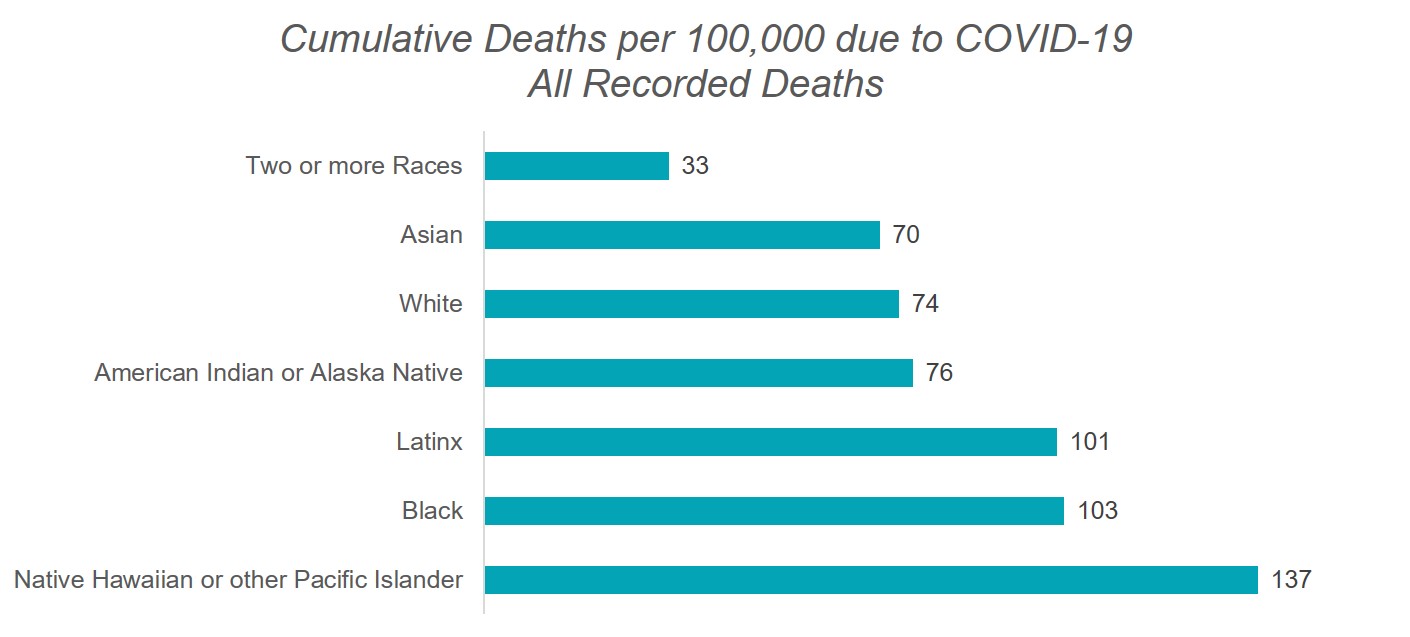
Deaths due to COVID-19 reveal further disparities among communities of color. Black, Latinx, and Native Hawaiian or other Pacific Islander communities all experience COVID-19 deaths at a higher rate than other groups. Although data for Asians suggests a lower death rate, disaggregated data that breaks apart the diverse ethnic groups classified as Asian is not available.
Source: U.S. Census Bureau American Community Survey; California Department of Public Health COVID-19 Race and Ethnicity Data; California’s commitment to health equity
People of Color Are Most Likely to Work in Industries Most Negatively Impacted by COVID-19

At the start of COVID-19 Stay at Home orders in March 2020, workers with “essential” jobs maintaining our societal infrastructure and operations were exempted from Stay at Home orders. Often these positions put essential workers at a higher risk of contracting COVID-19.
Communities of color hold the largest percentages of essential workers. The Latinx community is the largest group with front-line essential workers, with 55% Latinx people working in these positions. Among Black people, 48% are front-line essential workers while 37% of Asian people are front-line essential workers. White people have the lowest percentage of front-line essential workers at 35% of the white population.
Source: Front-line Essential Jobs in California: A Profile of Job and Worker Characteristics
Communities of Color Have Experienced Greater Rates of Housing Instability During the Pandemic
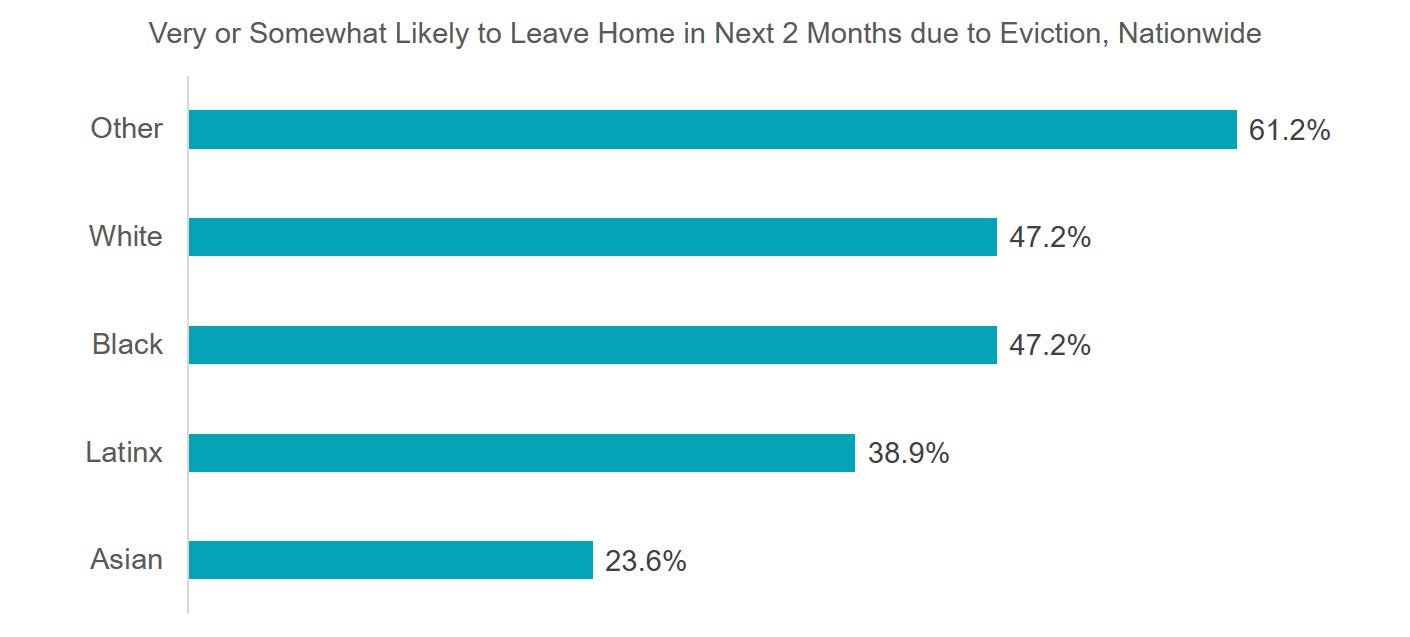
The Coronavirus pandemic has caused a significant increase in unemployment that has left families unable to pay their rent. Though there have been federal and state-based efforts to halt evictions, landlords can still file evictions against their tenants due to non-payment, among many other reasons. The pandemic has caused a wave of housing instability among communities of color. Nearly half of all Black tenants are very or somewhat likely to face eviction in the next two months. Only slightly behind are Latinx tenants with almost 40% and Asian tenants at nearly 25% of being very or somewhat likely to face eviction in the next two months.
Conclusion
Like the title of our publication confirms, there is an opportunity for advocates and community members to work together and address health disparities in California. With the disruption of the COVID-19 public health crises, the nationwide attention being drawn to historical racial harm and violence, and the start of a new federal administration, we should use this opportunity to rebuild our healthcare system’s foundations with the interests of communities of color in mind. For too long, the health and well-being of communities of color have been afterthoughts in the construction of our health care delivery systems.
In January 2019, the California Health Care Foundation funded the California Pan-Ethnic Health Network (CPEHN) to develop a set of policy recommendations on ways to more directly link health care payment and delivery reform efforts to promising strategies to achieve health equity. Briefly, our recommendations to achieving equitable care and health outcomes are interlocked facets currently missing in our healthcare system. We must center equity in quality and payment, engage patients’ families and caregivers, and strengthen culturally and linguistically appropriate care. System-wise, we must improve and integrate physical, behavioral, and oral health care, hold health plans and systems accountable, and improve social determinants of health.
Together we can assure we not only have a voice in the development of an improved healthcare system but are committed leaders in the movement for racial justice and health equity. We invite you to join us in this historic effort.